Professor Pierluigi Bove addresses a point that is often overlooked: after prostatectomy, spontaneous recovery of erections concerns only a minority of patients, and rehabilitation pathways are not always the most effective answer.
When pelvic oncologic surgery and quality of life are discussed, the focus is often placed on cystectomy. After bladder removal, the risk of losing erectile function is indeed high. But if we look at the overall numbers, there is another reality that affects many more men.
“The concept should be shifted from cystectomy to prostatectomy,” Professor Pierluigi Bove notes. “In terms of incidence and prevalence there is no comparison: prostate cancer is the most common cancer in men and its impact is clearly larger.”
This means functional recovery after surgery is not a niche topic. It is a central issue in everyday clinical practice, particularly when discussing radical prostatectomy.
The clinical point: not every patient is a true candidate for nerve-sparing surgery
In common conversations, erectile function is often assumed to “come back” after surgery, with time and some form of therapy. The reality is more selective.
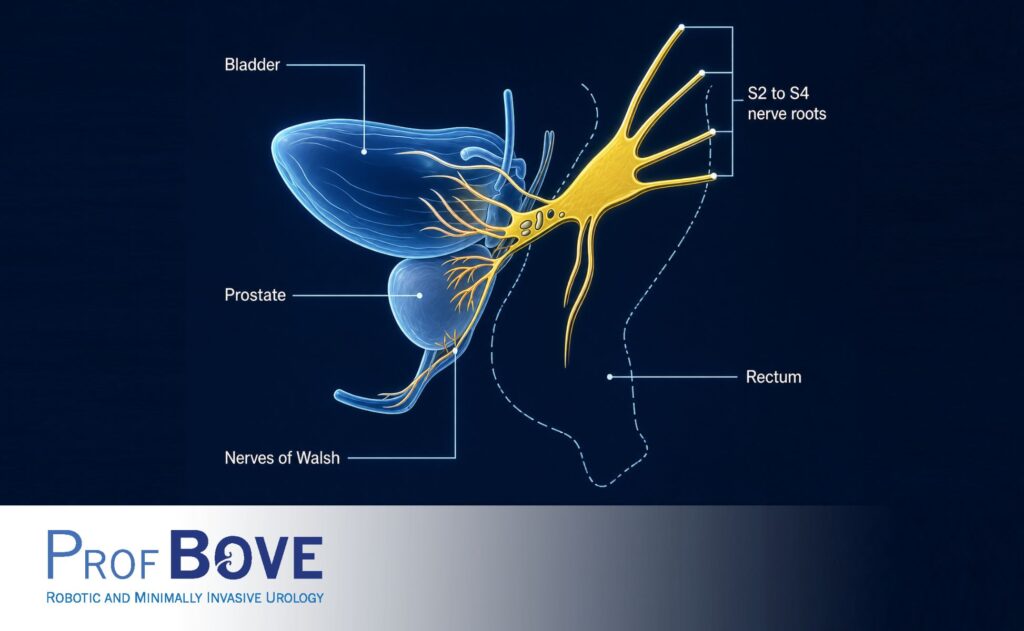
“The chances of recovering erectile function after prostatectomy apply to only a small group of patients,” Professor Bove explains. “We are talking about men who are truly eligible for a pure nerve-sparing or intrafascial procedure.”
In practice, this applies to a limited proportion of cases. Typically, these are low-risk—or at most favorable intermediate-risk—tumours with clearly localized disease. For many other patients, to achieve adequate oncologic control, part of the neurovascular structures has to be sacrificed.
The result is that, for a significant number of men, recovery is neither quick nor guaranteed.
“For many patients, surgery inevitably means that a portion of the nerves has to be removed,” Professor Bove stresses. “And that changes the probability of recovery completely.”
There is also a human and time-related aspect that is often underestimated. Early on, the patient is understandably dominated by the cancer diagnosis: fear of dying, concern about suffering, and a strong focus on “removing the tumour.” In that phase, functional complications—urinary incontinence and erectile dysfunction—inevitably move to the background.
But that balance changes over time.
After surgery, when the patient moves beyond the most critical phase, when follow-up is reassuring and a future perspective returns, other questions emerge. That is when erectile function becomes central to the patient’s perception of quality of life.
“That is often when the real ordeal begins.”
The patient may enter long pathways involving medications, injections, devices, repeated attempts, with expectations that are often high and results that are not always proportional. This gap between hope and reality can carry a significant psychological burden, leading to frustration, a sense of failure, and, in some cases, a depressive state.
When recovery happens, it often follows years of attempts
Structured rehabilitation pathways exist, including oral pharmacotherapy, intracavernosal injection therapy, vacuum devices, and other strategies. In some cases they are helpful. But it should be stated clearly that they do not always lead to a satisfactory recovery, and when they do, the timeline may be long.
“When these patients recover, they often do so after years of medical therapy, injections, vacuum devices, and more,” Professor Bove says.
This is not about denying the value of rehabilitation, but placing it in the right context: it is a tool, not a promise. And it should not be pursued by inertia, without a realistic assessment of probabilities and goals.
A different approach in selected cases
Clinical experience points to a simple idea: in some patients—especially when the chances of spontaneous recovery are low—it can make sense to discuss alternative options early, with a more concrete horizon.
“Translating the concept of a one-step approach to prostatectomy in patients with minimal or moderate nerve preservation can help avoid many psychological and functional problems,” Professor Bove explains.
Put plainly: rather than leaving the patient in a long and often frustrating sequence of attempts, it may be reasonable, in selected cases and with clear indications, to consider a more direct pathway that reduces waiting time and uncertainty.
One sentence Professor Bove repeats on this topic is very clear: “Enough with extremely expensive rehabilitation pathways that achieve little and, in many cases, lead the patient into depression.”
Without generalizing, the clinical message is that patients should be guided with realism. A topic this sensitive should not become an “afterthought,” managed with an open-ended sequence of trials without a strategy.
Clear information and shared decisions remain the core
Talking about erectile function after prostatectomy does not mean shifting attention away from cancer treatment. It means integrating the cure with what matters to the patient in real life, and doing so transparently.
Decisions about the functional pathway cannot be standardized. They depend on tumour stage and characteristics, the type of surgery that is possible, the patient’s baseline condition, and expectations. But one element should be constant: telling patients upfront what is too often discussed only later.
References:
prostate cancer, radical prostatectomy, erectile function after prostatectomy, post-prostatectomy erectile dysfunction, nerve-sparing surgery, intrafascial surgery, eligibility for nerve sparing, erectile recovery after prostatectomy, postoperative erectile rehabilitation, intracavernosal injection therapy, vacuum erection device, pharmacological therapy for erectile dysfunction, quality of life after prostatectomy, functional outcomes of prostate cancer surgery, doctor–patient communication, shared decision-making, urologic oncology Rome, Prof. Pierluigi Bove, Policlinico Tor Vergata, URMI, UPMC